I’m currently on a 2-week rheumatology “selective” (A select elective- someone thought they were being very clever when they came up with that one!). From a list of about a dozen medical specialties, I ranked Rheumatology fairly highly and it’s the specialty that was assigned to me during the lottery. I’m going to guess it’s not a very popular selective amongst third year, as I’m the only medical student out of 6 rotations in our clerkship that will be rotating through the rheumatology clinic (GI, telemetry, and cardiac critical care seem to be the top picks for most medical students- 12 students are doing electives in each of those specialties over 3 months, I’m the lone student in rheumatology!). Be that as it may, I was personally very happy to get assigned to rheumatology, though I’ll be honest and say that I wasn’t exactly sure what I would be seeing on the service…
Rheumatology is a sub-specialty within internal medicine focused on the treatment of… rheumatological disorders. I’m not trying to be obtuse, but while hepatologists treat the liver, nephrologists treat the kidneys, and cardiologists treat the heart, rheumatologists don’t really have an organ (or an organ system like gastroenterologists or endocrinologists) of focus. Instead, rheumatologists treat arthritis, autoimmune diseases (the ones that others don’t want to claim- Type 1 diabetes, for example, is treated by endocrinologists, Multiple Sclerosis is treated by neurologists), and pain disorders. Rheumatologists spend a lot of time with clinical problems involving joints and soft tissue, but the conditions they treat can also manifest as vasculitis (inflammation of the blood vessels), fibrosis, or just about anything. The common thread that ties together rheumatologic disorders is some component of autoimmune dysfunction- the body attacking itself.
You would (correctly) assume that rheumatologists see a lot of people with rheumatoid arthritis, but they also are the clinicians that get the most puzzling “WTF?!” cases. Rheumatologists treat people with Lupus, Sjögren’s syndrome, Reynaud’s phenomenon, sarcoidosis, scleroderma, a host of other rare and mysterious disorders, and a number of people who obviously have something “wrong”, that no one can quite label. If you’re in the medical profession and you have a confusing case, lupus is almost always somewhere on the differential diagnosis. If you’re a House MD fan, you might think “It’s never lupus”, though of course it sometimes is!
Treating rheumatological diseases is difficult. Depending on the diagnosis, there may be no recognized treatment or many pharmacological interventions. Unfortunately, while some of the drugs work for some of the people with some of the conditions, there are many people who reap no benefits from pharmacological intervention. Also, as the drugs that are used to treat these disorders are generally meant to suppress the immune system, treatment often comes with unpleasant side effects. It is generally believed that you cannot “cure” rheumatological diseases- you can treat, mitigate, and hope for remission, but a diagnosis of lupus (or any other rheumatological diagnosis) is a lifetime diagnosis.
There is a real paucity of understanding of the pathogenesis of rheumatological diseases. It is generally recognized that there is a genetic predisposition to these diseases, and some are associated with specific HLA markers. However, not everyone who gets these diseases has a known marker or a family history, and not everyone with a family history or a known marker gets disease. There is a lot of research being doing exploring the pathogenesis of a number of these diseases (though some are very rare diseases, and as such are rather understudied and under-explored for pharmacological intervention), but there have yet to be any great breakthroughs in their understanding. (To give you an idea of how poorly understood these conditions are, check out the PubMed page on Lupus – everything is very vague!)
I do not pretend to have a deep knowledge of rheumatological diseases, nor am I particularly well versed in the research that has been conducted exploring these conditions (it is definitely not my field of expertise), but my experience, my clinical education, and my academic pursuits have led me to suspect that many of these diseases are the result of the increasing mismatch between our evolutionary past and our modern world.
It appears to me that many rheumatological disorders (though probably not all), are caused by a 3-pronged attack. First, there is a genetic component that makes some individuals prone to disease. This is likely a component of the immune system that, when presented with an evolutionary-novel antigen, turns the immune system on in a way that leads to an auto-immune response. Or it might also be a non-immune system component that is an epitope that is targeted by our immune system after it has been activated by an evolutionary-novel insult. While viruses have been implicated as the source of some of the inappropriate activation of our immune system, it seems to me that the gut is likely a greater source of disorder for many individuals. In the presence of the second contributory factor, a leaky gut (as I discussed briefly in my post on Liver Saving Saturated Fats), novel antigens from the diet are able to make their way into the body where they can activate the immune system in susceptible individuals. This is probably magnified by the third major contributor- our immune system built for another time. Our immune system has evolved significant gun-power to keep us safe from the parasites and microbiota that occupied our body through the course of evolution- in the absence of an appropriate opponent (helminths or otherwise), and in the presence of a novel target that looks a bit like oneself, the immune system turns on itself.
These are the basics of my thought process on an evolutionary approach to rheumatological diseases, although this argument should be expanded to include the role of Vitamin D (indeed, it appears Vitamin D levels are inversely correlated with the risk of developing and the severity of symptoms of rheumatoid arthritis [1]), the role of cortisol and stress on the immune system, and other factors that effect gut permeability such as stress and high intensity exercise (dietary factors tend to be most frequently implicated in problems of gut permeability).
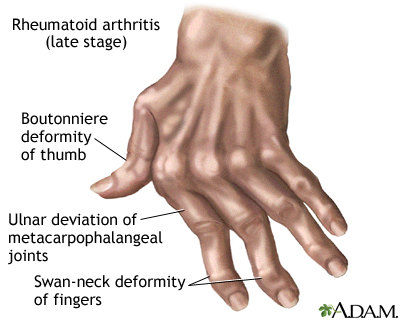
So how does this hold up? Well- to my knowledge, there hasn’t been any research exploring the effects of an evolutionary-appropriate lifestyle on rheumatological conditions (and, as with so many conditions, one always has to consider what type of results you might see with a lifestyle intervention when disease is already present, instead of trying to prevent disease from the get-go). What I can say from my experience in rheumatology clinic is the following- with rare exception, the patients with rheumatological disease look sick (and I’m not talking about the tell tale signs of rheumatoid arthritis). They are pale, they look tired, they report being fatigued, they get little sleep (and that which they do get is very poor), they are frequently very overweight, and they are very stressed. I’m not saying that these factors cause the disease (and in some cases the disease probably causes the other problems), but it is additional evidence that the patient is unlikely to be living an “evolutionary appropriate” lifestyle.
In my readings, I did come across an interesting paper [pdf] that looked at the prevalence of rheumatological disorders in Australian Aboriginals. I’m not surprised (and I hope you’re not either), that
“No evidence was found to suggest that rheumatoid arthritis (RA), ankylosing spondylitis (AS), or gout occurred in Aborigines before or during the early stages of white settlement of Australia… Since white settlement, high frequency rates for rheumatic fever, systemic lupus erythematosus, and pyogenic arthritis have been observed and there are now scanty reports of the emergence of RA and gout in these original Australians.” [2]
In contrast, it appears that indigenous people are currently more prone to rheumatological disorders [3]. This does not surprise me, as the factors that likely cause these diseases have been thrust upon these populations in the course of one or two generations, unlike the gradual decline of the “civilized” lifestyle that some of us may have some evolved resistance against. Disappointingly, researchers seem to be more interested in exploring genetic predispositions, rather than the lifestyle factors that are likely the drivers of disease.
So what is there to do? Firstly- I feel that people with rheumatologic disorders would greatly benefit from an ancestral approach to health. This includes, but is not limited to: an evolutionary appropriate diet, adequate vitamin D (ideally synthesized endogenously from sunlight exposure), sleep, stress management, and movement. Does this help? It certainly appears to, judging from the N of 1 experiences that dot the internet:
Here are some success stories:
Rheumatoid Arthritis via Robb Wolf
Lupus via Julianne Taylor
Takayasu’s Arteritis via The Domestic Man
Much as when I wrote about my experience with psychiatry, I feel like rheumatology patients are a population that lack a voice. People “get it” when you have a kidney problem, or a heart problem, or even if you have a back problem, but people don’t seem to believe that the symptoms that a rheumatology patient experiences are real. They hurt, but why? They have joint pain, but why? Even with our patients- some seem to (sadly) accept that this is their lot in life, but many want to know why. The answer, it seems to me, is that these are people whose bodies react in a violent manner to the mismatch of our modern world with our evolutionary expectations.
My hope is that, by looking at disease through the lenses of evolution and in the context of ancestral peoples, rheumatology patients (and others) can be steered towards a lifestyle that takes our evolutionary history into consideration. We don’t have to forsake the comforts of the modern world (and we should take advantage of modern medical advances!), but perhaps we could all find a better balance of exercise, sleep, nutrition, and lifestyle for our health, and for our happiness.
1. Song, G.G., S.C. Bae, and Y.H. Lee, Association between vitamin D intake and the risk of rheumatoid arthritis: a meta-analysis. Clin Rheumatol, 2012.
2. Roberts-Thomson, R.A. and P.J. Roberts-Thomson, Rheumatic disease and the Australian aborigine. Ann Rheum Dis, 1999. 58(5): p. 266-70.
3. Peschken, C.A. and J.M. Esdaile, Rheumatic diseases in North America’s indigenous peoples. Semin Arthritis Rheum, 1999. 28(6): p. 368-91.

{kind=link}
Excellent. May I make a suggestion vis-a-vis methods and analysis? Understanding the nature of your training program, it looks as if the epistemology leans heavily toward allopathy, likely excluding exercise physiology both in theory and practice.
Arthritis is not a singular noun, rather descriptive of more than 80 conditions! Now that’s a hot topic for upstream causality other than over reliance on the fashionable ‘my genes (or the devil) made me do it.’ Soft tissue is definitely involved, and there’s an exceptionally fine line between arthritis and tendonitis.
Genomic and proteonomic based exercise physiology favors looking at the Sedentary Death Syndrome for gaining a sense of upstream causal factors. In a genomic model, arthritis is not a stand alone condition, rather something to be viewed and analyzed within the whole system. In that regard, arthritises (plural) are outcomes, not state specific diseases – ie, symptoms of deeper stirring metabolic erosion.
In my limited experience, considerable success has occurred with morbidly obese women with painful arthritic knees. Obesity by itself is far from what has to be taken into account. Beneath those rippling mounds of packed in stored energy (bodyfat – even thunder thighs!) reside exceptionally atrophied leg muscles – indicating loss of type II fiber, associated neural tissue, presumably some stage of osteoporosis, and loss of connective tissue. Same persons have ‘bad backs’ – indicating posterior kinetic chain is likewise in trouble. All things considered, combining loss of strength with increased demand for strength, their knees and hips are taking the hit – neither the well equipped shock absorbers and bearers of burden that are skeletal muscle. Add to that the skeletal muscle’s own unique biochemistry, rendering it part of the endocrine system.
I’ve generally put such patients on programs of high rep stage sets three times weekly. Generally within six weeks reporting indicates incredible reduction of arthritic symptoms. High rep stage sets promote far more rapid hypertrophy than any other method. Unfortunately, the dominant paradigms of ‘sports medicine’ have not considered sarcoplasmic hypertrophy much to their dismerit.
Physical rehabilitation of joints is definitely important, but it’s more of an issue for orsteoarthritis than rheumatoid arthritis. That being said- other than generally thinking “strength is good” I’m yet to do the Physical Medicine and Rehabilitation clerkship where I will hopefully learn more specifics of rehab.
here’s another one. http://exceptionallybrash.blogspot.com/search/label/autoimmune
Thanks for sharing.
I so appreciate your compassion towards patients whose symptoms are often vague and lack a clear diagnosis. It can be genuinely *embarrassing* to go to a health care professional over and over with symptoms that don’t have a clear cause and seem to bleed into each other. One starts opening conversations with justifications like, “Please, I’m not depressed, and I’m not under any unusual stress, but…”
Increasing my vitamin D level from very, very low to only borderline (still working on that) has made a huge difference in my life. It’s given me the luxury of changing other lifestyle aspects. It’s hard to wash and chop endless fresh veggies when Raynaud’s and unspecified joint pain are a constant problem, or to increase physical activity when there’s extreme fatigue and yet more pain. … And my disease (um, whatever it really is) was so mild compared with many people’s… I hope that the changes I’ve made keep it that way for many, many years to come (despite family history and my own past).
I’m glad to hear that you’ve found some lifestyle interventions that improve your condition, and I hope that you continue to find more.
I can only imagine the frustration of having a complex disease and being seen in a busy primary care office with a physician without much rheumatology background. Even in the setting of a good rheumatology clinic, patients can become frustrated trying to describe their myriad of symptoms.
Great post! I’ve been dealing with Rheumatology since my diagnosis of Takayasu’s Arteritis in 2006, and I can attest to the “Dr. House” idea – my first Rheumatologist was introduced as “our hospital’s House”!
I’m also interested in hearing about successes with an ancestral lifestyle following diagnosis, as opposed to prevention of rheumatological symptoms; I’ve been eating ancestrally for about two years, and have definitely found some success. Specifically, I was able to discontinue one of the three immunosuppressants I’ve been on since diagnosis, and increase my level of exercise – and I’ve managed to significantly minimize my typical auto-immune symptoms (fatigue and bad sleep in particular).
Russ- thanks for commenting, and for reminding me of your story- I have added it above.
I think “success” is a very subjective thing, especially with rheumatological disorders. While we may all hope for a complete remission of disease, being able to remove one drug or improving someones ability to live a somewhat normal life is a massive success.
I would love to see a trial where lifestyle was used to treat rheumatoid disease, but of course there are so many difficulties. First there is the heterogeneity of rheumatoid diseases themselves, then there are so many variables to consider when you make “lifestyle changes”. That’s not to say it can’t be done, and I’m enthused to see people like Terry Wahls doing trials looking at the effects of a whole diet modification (instead of, say, an O3 supplementation) on a condition such as MS.
And don’t forget earthing. Probably the aborigines have started wearing shoes and living in houses that are electrically insulated from the ground. That has deprived them of the beneficial effect of electrons that cover the earth. 2 links will illuminate this factor:
http://www.earthinginstitute.net/
http://naturesplatform.com/earthing.html
Actually many aborigine who don’t wear shoes often or indeed have houses, will have these health problems that were unknown in the dreamtime.
Here are some anecdotal reports of lupus cures by earthing.
http://curezone.com/forums/am.asp?i=1816961
http://www.earthinginstitute.net/index.php/site/blog/Earthing_Institute_Reports/
Still anecdotal, but research is very expensive and I don’t expect the NIH to fund such studies anytime soon.
Here, FWIW, is my ideas on lupus; lupus is associated with salicylate intolerance, http://www.lupuswa.com.au/aboutlupus/complementarytherapies.html
and many drugs can aggravate lupus.
http://en.wikipedia.org/wiki/Drug-induced_lupus_erythematosus
These drugs and salicylates share a common detox pathway; CoASH conjugation and S-acetylation.
Hence this old treatment: http://www.ncbi.nlm.nih.gov/pubmed/13180024
However, pantothenic acid deficiency alone isn’t a very likely cause. What else would reduce CoASH?
Sulfur deficiency, and a low-fat diet. Carnitine deficiency might also limit Co-ASH synthesis. This might explain why lupus seems to be more prevalent in educated women, who are perhaps more likely to go to extremes of low fat, low sulfur protein eating while increasing salicylate intake.
I am thinking a high-fat paleo diet, pantethine or B5, NAC or Taurine, B12 and acetyl carnitine.
Interesting comments. I think your point about a low fat diet being a potential culprit is interesting (and in my mind I also implicate a low fat diet with a number of other conditions, though I haven’t put the thought and reading into fleshing this into a blog post yet).
Rheumatological disorders (like many psychiatric disorders, actually) are not clear and definitive diagnoses. Blood tests can be suggestive of a diagnosis, but there is a lot of heterogeneity within each disease, both in presentation and diagnosis. Anti-Smith antibodies, for example, “give you” the diagnosis of Lupus, but only a fraction of patients with diagnosed Lupus have positive anti-sm antibodies. Like so many of our modern diseases, I doubt there is truly one “cause” of these diseases, unless you back out of the picture so broadly to make a blanket statement such as “a genetic predisposition in the context of an evolutionarily-inappropriate lifestyle”. I think that a number of factors (deficiencies and stressors) are likely of varying importance for different patients.
A nutrient dense diet is definitely an appropriate approach to managing rheumatologic disorders (at least in my mind). I think that the success Dr. Terry Wahls has had with her diet recommendations in the context of patients with MS (also autoimmune) is very encouraging.
(Broadly- sorry I haven’t commented back to everyone’s comments- I do appreciate them, but don’t necessarily have time to get back to them all!)
To connect this hypothesis with the autoimmune nature of Lupus, consider the wide range of proteins that are activated or de-activated by acetylation:
http://www.cellsignal.com/reference/pathway/Protein_Acetylation.html
Is it possible that underactive N-acetylation or S-acetylation results in one or more of these proteins malfunctoning in immune cells, or becoming a non-self mimicking target in other cells?
Intriguing references online to N-acetyl glucosamine being beneficial in Lupus, but no research I can find in a quick search.
P.S. a book well worth reading on autoimmunity and allergies; “an epidemic of absence” by Moises Velasques-Madoff; the latest news from the Hygiene Hypothesis front.
So if you think that gut is the prime cause of illness then we can divide the problem. The obvious points of action are agricultural foods, drugs and food industry related stuff.
1. Microbiota changes in constitution and behavior relative to ancestral flora.
1.1. Agri: Dominant usage of wheat and friends leads to leaky gut (via zonulin pathway) which let microbiota enter the system.
1.2. Drugs: main suspects are antibiotics and antacids, each changing microbiota profile (killing protective flora, selecting for resistant steins, reducing acid barrier ….)
1.3. Food industry “addons” like zero fat, high carbs products, which lead to SIBO, attenuated immune system because of vitamin C competition and malnutrition leading to altered profile in the gut.
2. Malnutrition:
1.1. Dominance of specific foods with anti-nutrients.
1.2. Drug induced malnutrition.
1.3. Stealing by microbiota (h pylory etc.)
1.4. Collateral damage from auto-immune processes to enteroc. and friends.
Ancestral diets are unlikely to be optimal solution becuase there is no such thing unless somebody discoveres time travel. Food profile has changed, and unless you own a cow and a land the probability that you will be ancestral is very low.
I think the best action to take is appropriate mega-vitamin therapy combined with surrogate of ancestral diet. This also has potential to fix other causes of disease (genetic ones for instance).
Your notion that vitamin D should be obtained via sun exposure misses a big problem: there is an upper limit in production, it also depends on dietary cholesterol and other resources, drugs (statins for instance), and due to industrial changes in last century sunlight is much stronger then before and hence its cancer inducing effect comes as a problem. Far better option is to use supplement and probably megadoses as a treatment (showed results for scleroderma for instance, and various other auto-immune disorders). That sunlight may not be enough for specific people (depending on race and skin tone for instance) was obvious for me when I checked my levels after 30 days on the beach after 1 year of >10 000IU per day and 20 minutes of sunbathing each day during that year (~10% of the body) [ also including other synergistic nutrients like Mg and K2] where I was still insufficient after that. I would suggest some quality Cod liver oil as the best way to get ‘natural’ vitamin D (with added benefit of the best form of vitamin A which itself will help with joint problems because of it anti-obesogenic potential in higher doses).
Anyway, it works for me, the way I described it, for now. I solved around 10 chronic problems (obesity, scleroderma, eczema, constant infections, hemorrhoids, constant dental problems, strange allergies etc..).
When I told my rheumatologist that my symptoms come and go as I eat and avoid gluten she was genuinely surprised as she never heard about that. That is the kind of healthcare you get.